Empowering caregivers and family members with information access and answers to their questions about long-term care.

St. Joseph’s Lifecare Centre is a not-for-profit long-term care (LTC) home located in the City of Brantford. Our team was tasked with developing an innovative design-thinking project that would best serve the caregivers and family members of residents; while also positively setting it apart from the other long-term care homes in the area.
How might we enrich the experiences of caregivers and family members of residents at St. Joseph's Lifecare Centre?
While most group members had general knowledge about Ontario’s long-term care system and its functions, there was much more to learn about this ecosystem and the groups involved. At the centre of this project, caregivers and family members were our core focus for a user-group.
Using an ecosystem map helped to visualize the different user groups, their roles within the LTC system, and how they interact and relate to one another.

We conducted one-on-one interviews (n = 9), a focus group (n = 5), and an observational study (n = 1) to better understand the following from caregivers and/or family members of residents
The research was conducted in-person at the Brantford location of St. Joseph’s Lifecare Centre. Through a combination previously agreed upon participation in our research and the recruitment of participants from a drop-in basis, the participants were all (at some point) a caregiver and/or family member to someone in long-term care.

From the generative research, what stood out was the overwhelming concern and frustration with caregivers and family members’ past experiences. These experiences and their contributing factors related to long-term care, but could not be controlled by St. Joseph’s or any long-term care home. This included long-wait lists, facilitated by Home and Community Care Support Services / Local Health Integration Networks (LHIN) and determined by placement priority categories outlined in the Fixing Long Term Care ↗ Act of 2021. Caregivers and family members also expressed concerns about short-staffing and its affects on the quality of care provided to their loved one.
In Ontario’s not-for-profit LTC homes, “there is no legislated minimum staffing ratio (the number of nursing home staff members compared to the number of residents), and no legislated requirements related to how much care residents receive on a daily basis” (Registered Nurses' Association of Ontario, 2018)
However, there were some addressable issues and concerns that caregivers/family members brought up during the generative research phase. Two of the most notable categories concerned communication, and their feelings and emotions.
Communication:
Feelings and Emotions:
From the synthesis of the data gathered from the generative research phase and the secondary research conducted (competitive analysis and literature reviews), four archetypes were created and used to map out the user needs, their pain points and goals.
This service blueprint helped to visualize a typical end-to-end visit at St. Joseph’s, including the interactions and tasks required by visitors to the LTC home. It was also useful to highlight the over-reliance of PSWs and RPNs for basic information accessing tasks.

The ideation phase brought all sorts of ideas to the table, many of which were not in the scope or control of our client.
We sought to visualize the different avenues that our solution could incapsulate including marketing and outreach campaigns, improved feedback systems, new communication channels, and intentional peer-support programming.
In this first (of two) ideation phases, the team brainstormed potential solutions that could address the different problem areas and pain points identified.

The Caregiver-Resident Board aims to facilitate communication and serve as an additional method of information sharing between caregivers, family members, residents and the long-term care home staff.
Ideally placed in the room of each resident, each board is customizable based on the communication needs and comfort-level of the resident and family. This preliminary iteration features a hybrid-display, chosen for its flexibility in conveying both dynamic and static information and in being a middle-ground for the varying levels technological proficiency in the anticipated user group.
The digital display would show dynamic information that regularly changes (staff on shift, meal offerings, activity schedules, etc.).
The middle board would be used to share preferences and personalized information about the resident, to help staff better connect with them and to keep them up to date. The right-most board would be used to establish and document communication between caregivers/family members and staff.

At a high level, the proposed Caregiver-Resident board would instead centralize access to all this information (and more), and facilitate its access from every resident’s room with reduced barriers to access.
In presenting this solution and its features to the client, they noted similarities to existing methods and procedures in place at the LTC home that likened to our proposed solution. The high-level similarities and overlaps mentioned in the client meeting are illustrated below.
Note: Real pictures could not be featured due to privacy concerns.

A 8.5x11'' printed calendar of activities and events posted on a cork board in each resident's room.

Whiteboard with the names of front-line staff currently on shift. Displayed at the nurses’ station on each wing of the LTC home.

TVs outside of each wing and the dining room displaying the daily menu.

A 8.5x11'' printed weekly menu displayed on a door near the dining room.
Examples provided by the client indicated that those methods served and prioritized access for the front-line staff on shift, and did not adequately serve the caregivers/family members–as noted through data aggregated during the generative research phase.
With further discussion and evaluation, the team learnt that the crux of the Caregiver-Resident board were the policies and procedures dictating feedback processing: whenever a feedback form is received, the contents of the feedback form are formally filed as a complaint, regardless of the nature of the issue (information seeking, small question, major concern or complaint, etc.). For the client, a major non-negotiable functional requirement was a system that would not increase workload for members of upper management.
Based on client feedback, we stepped back from the proposed hybrid communication board; sparking a flash round of ideation wherein we decided to hone-in on a digital solution.
Despite the time crunch, it was vital that our revised solution was still driven by the data collected from our user research.
In our rapid ideation session, the team made sure to refer back to themes, quotes, and other participant informed artefacts from user research sessions.


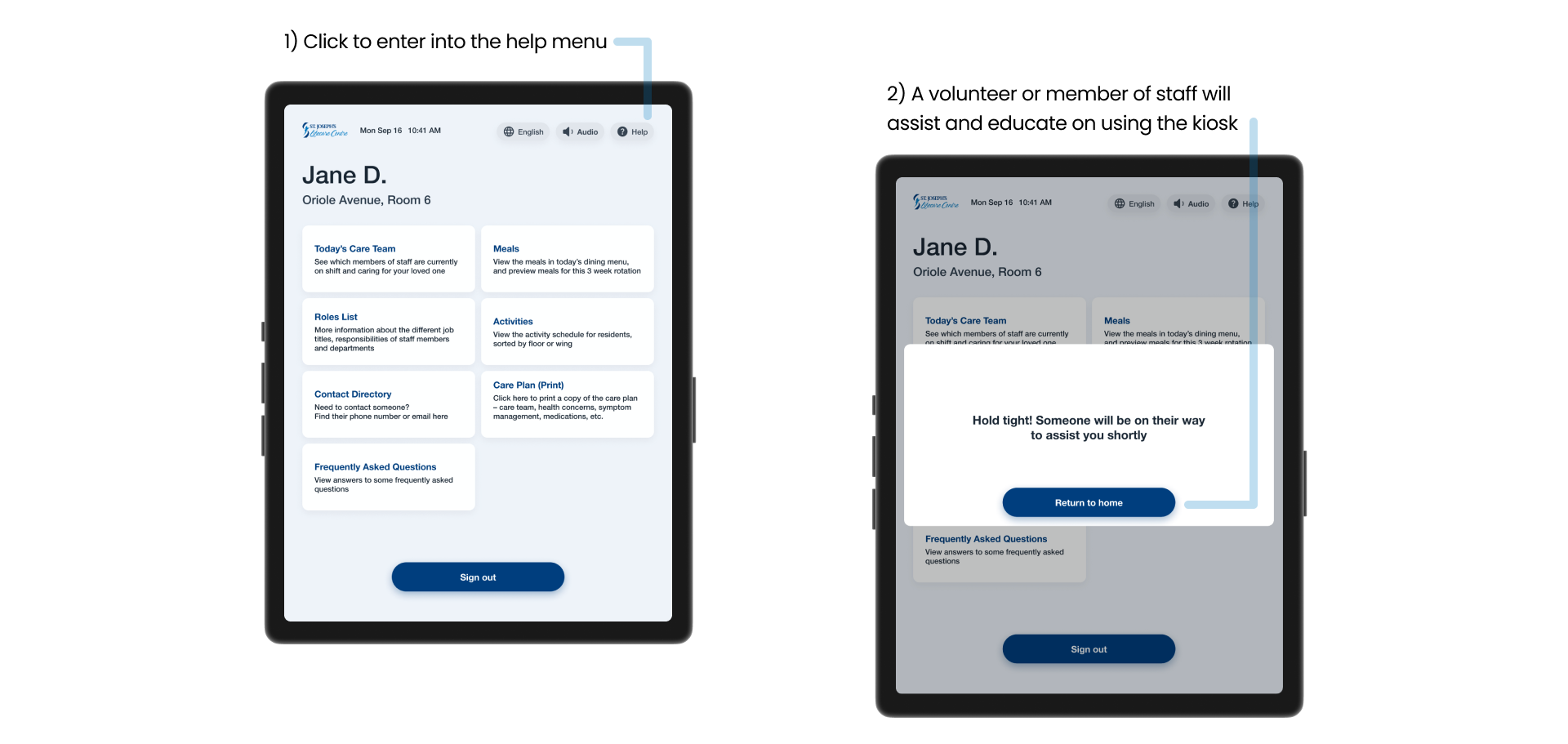
The v2 kiosk prototype was a low-fidelity mockup designed in Figma.

We held drop-in sessions to elicit feedback from caregivers and family about our proposed kiosk solution. After being briefed on our project, research objectives, and obtaining consent to participate, we asked participants (n=5) to envision themselves using the kiosk to complete tasks in the following scenarios.



Positive Informative Insights
Constructive Criticism
Taking account of the changes from the low-fidelity testing, the medium-fidelity prototype was updated in Figma. This round of usability testing required participants (n=6) to complete four tasks using the kiosk interface.
In teams of two, the kiosk interface was presented to participants on an iPad. The usability testing included four tasks that sought to inform researchers if the caregivers/family members could navigate the interface.
Metrics like completion (fail, succeed, or indirectly succeed), number of errors (misclicks, wrong paths traveled, etc.) and approximate time on task were measured by researchers. A combination of iPad screen recording and visual observation were used to note participants' thoughts and actions.
Tree testing allowed us to understand our users' mental models and evaluate whether the system design matches their understanding. In this unmoderated tree test, participants (n=7) were presented with two tasks. These tasks were reframed from the two poorest-scoring tasks presented in a previous usability test.


The aim was to gain insight into how users expect information to be organized, to test the effectiveness of the labelling, the organization of information and retrievability of information resources found within in the kiosk’s medium-fidelity navigation system.
From the information architecture (IA) testing, we concluded that we should rework the labels and add more context to the upcoming page content.






It was honour and privilege of being able to interview, chat with, and learn about their stories and experiences at St. Joseph’s and within the broader LTC system. I’ve gained a much greater appreciation for all the caregivers, family members, front-line LTC staff members and the impactful and important work that they do. Throughout this design thinking project, I got just a glimpse into the complexity, vast and diversity of stakeholder involvement, and how real UX projects unfold.
My team and I are excited with the prospect of continuing this project and further developing it with consultation with upper-management. The next steps of this project will require further consultation with St. Joseph’s and other primary stakeholders to review the feasibility of implementing this proposed kiosk system.